📖 Read more: Xenotransplantation: Animal Organs in Humans
The Transplant Crisis
Every minute, somewhere in the world, someone dies waiting for a transplant. Waiting lists stretch for years. Kidneys are the most sought-after organ: thousands of patients endure exhausting dialysis sessions three times a week while waiting for a donor match that may never come. Bioprinting promises a future where organs are manufactured, not donated — built from the patient's own cells, eliminating both scarcity and rejection.
How Bioprinting Works
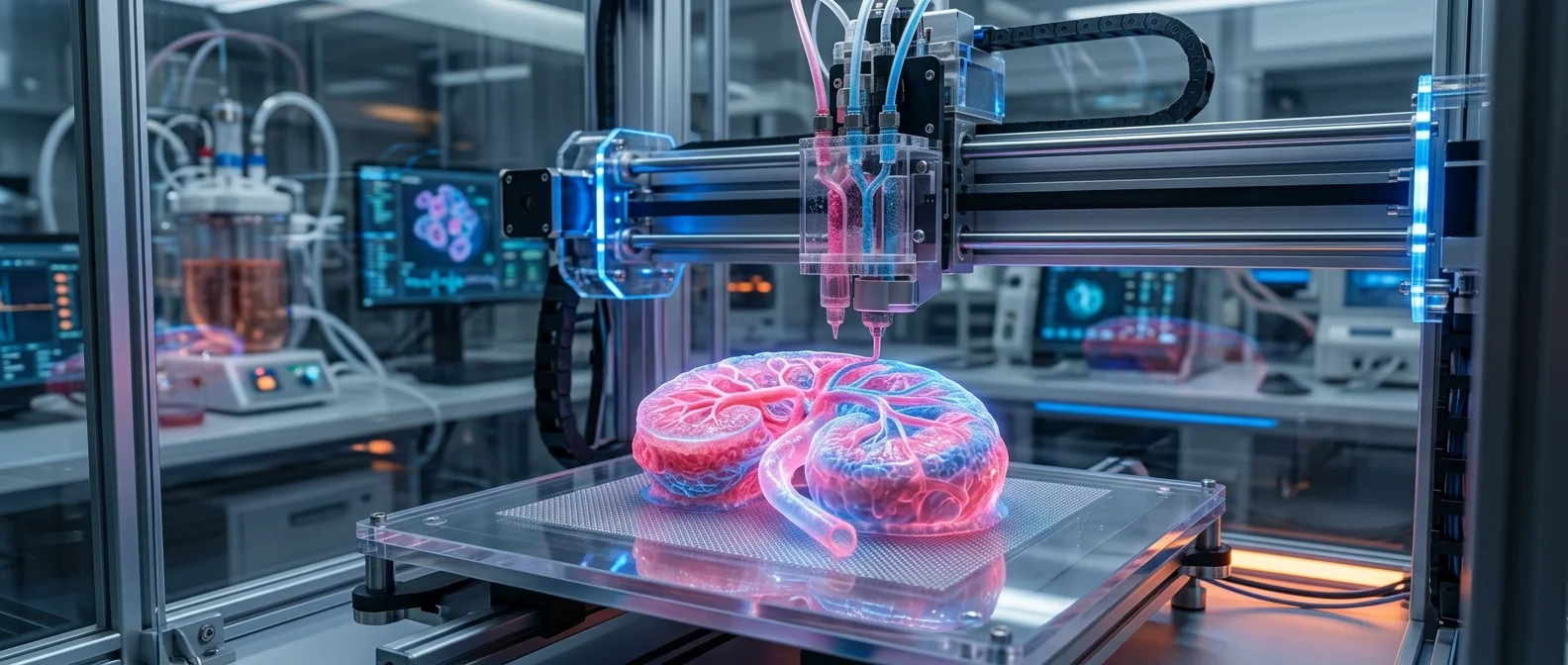
The principle mirrors an ordinary inkjet printer. Instead of ink, however, a bioprinter uses bioink — living cells suspended in a microgel made of gelatin enriched with vitamins and proteins that keep the cells alive. Instead of paper, the printer deposits layers onto a platform, building the organ layer by layer while an elevator gradually lowers the surface underneath.
The workflow for a custom organ starts with a CT or MRI scan of the patient. Those images are loaded into CAD software to create a three-dimensional model. The model is sliced into cross-sections, each mapping the precise placement of different cell types. The file is then sent to the bioprinter, and the organ is printed slice by slice.
From scan to organ: CT/MRI scan → 3D CAD model → Slicing into cross-sections → Bioprinting with bioink + microgel → Incubation → Living tissue. Liver cells, for instance, form tight junctions with each other and survive up to 40 days in the lab.
For simple organs like the bladder (only 2 cell types), the approach is relatively straightforward: print a biodegradable scaffold, coat it with the patient's cells, let it mature for eight weeks, and implant. For complex organs like kidneys and livers, the three-dimensional structure with many different cell types makes a bioprinter essential — no scaffold alone can recreate that complexity.
Milestones That Changed Everything
The story of bioprinting begins in 1983, when Charles Hull invented stereolithography and founded 3D Systems in 1986. The logic was simple: if a printer can build a plastic car part, why not an organ from cells?
- 1999: Wake Forest prints a synthetic bladder scaffold, coats it with patient cells — successful transplant
- 2002: A miniature functional kidney is printed that filters blood and produces urine in an animal model
- 2010: Organovo prints the first blood vessel
- 2012: The University of Michigan prints a tracheal sleeve for a baby with a rare condition
- 2024: WFIRM receives $48 million in funding for body-on-a-chip technology
The Wake Forest Institute for Regenerative Medicine (WFIRM), led by Anthony Atala, MD, remains at the forefront. With more than 550 scientists and collaborations with over 500 organizations worldwide, the institute is developing more than 40 different tissues and organs. The team has applied 17 different cell/tissue therapy technologies to human patients — including skin, urethras, cartilage, bladders, muscle, and kidney tissue.
Current Applications
A full-size organ printed from scratch has not yet been transplanted into a human. That doesn't mean bioprinting isn't already saving lives. Today's applications are striking:
- Skin grafts: WFIRM has developed a portable system that scans a wound and prints skin directly onto the patient. The goal is portable printers deployed in military field hospitals
- Ears and tracheas: Print a mold from a 3D scan, inject cartilage cells and collagen, incubate, and implant
- Bones and jaws: Doctors in the Netherlands implanted a 3D-printed lower jaw made of bioceramic-coated titanium
- Drug testing: Organovo prints microscale models of liver, kidney, and tumor tissue for drug testing — organs-on-a-chip that respond like real tissue, reducing reliance on animal testing
The Biggest Hurdle: Vascularization
The largest technical barrier isn't printing cells. It's vascularization — creating the network of microscopic blood vessels that supply every cell with oxygen and nutrients. Without capillaries, a printed organ dies within hours as its inner cells are starved of sustenance.
Current bioprinting technology can create larger blood vessels, but capillaries — vessels one cell thick — remain beyond the resolution of today's printers. This is the central challenge: without a solution to vascularization, fully transplantable organs stay in the future.
The Road to Kidneys on Demand
The journey from bladder to kidney is exponentially harder. A bladder contains two cell types. A kidney contains dozens, organized in a complex three-dimensional architecture threaded with a dense vascular network. This is why kidneys are the Holy Grail of bioprinting.
Combined approaches — bioprinting together with the patient's own stem cells, gene editing, and nanotechnology — offer hope. In January 2025, WFIRM joined a project aiming at whole eye transplantation, a challenge that blends bioprinting with regenerative medicine in uncharted territory. The road is long and uncertain, but every year brings scientists one step closer to the moment when “kidney on demand” becomes medical reality.
HowStuffWorks – How 3-D Bioprinting Works
Wake Forest Institute for Regenerative Medicine – WFIRM: A Leader in Translating Discovery into Clinical Therapies